The Genicular Nerve Block for Knee Pain in the Emergency Department
Maria Eberle, MD
Emergency Ultrasound Fellow, Department of Emergency Medicine, Maimonides Medical Center
Farnam Kazi, MD
Emergency Ultrasound Fellow, Department of Emergency Medicine, Maimonides Medical Center
Kaulin Ervin, DO
PGY1 Resident, Department of Emergency Medicine, Maimonides Medical Center
Jennie Xu, MD
PGY2 Resident, Department of Emergency Medicine, Maimonides Medical Center
Irina Sanjeevan, MD
Ultrasound Faculty, Department of Emergency Medicine, Maimonides Medical Center
Leily Naragi, MD, FACEP
Ultrasound Fellowship Director, Department of Emergency Medicine, Maimonides Medical Center, Assistant Professor, Emergency Medicine, SUNY Downstate Health Sciences University
Errel Khordipour, DO
Ultrasound Faculty, Department of Emergency Medicine, Maimonides Medical Center
Introduction
Patients regularly present to the emergency department (ED) with knee pain. As emergency physicians increasingly incorporate ultrasound-guided nerve blocks into their practice, the genicular nerve block may be a useful new technique for knee analgesia in the ED.
The genicular nerve block was originally described in regional anesthesia literature for the treatment of chronic knee pain and more recently described for knee analgesia in peri- and postoperative settings.1-4 Anesthesiologists use this block in conjunction with or in lieu of the femoral nerve block and the adductor canal block for various lower extremity pain control needs.5
The genicular nerve block spreads local anesthetic around three branches of the genicular nerve that innervate the knee joint capsule.1 This preserves quadriceps muscle strength by targeting only sensory afferents from the knee joint.3 Ultrasound allows for visualization of bony landmarks and other structures while performing the genicular nerve block in a point-of-care setting.
This block is shown to be safe and effective for achieving durable, motor-sparing, and opioid-sparing analgesia and employs similar techniques to other ultrasound-guided nerve blocks familiar to emergency physicians. Recently, a case report described the use of the genicular nerve block in an ED setting for a tibial plateau fracture where it provided effective analgesia for acute traumatic knee pain.6
Anatomy
The innervation of the knee joint and capsule is complex, and it is generally divided into the anterior and posterior compartments. The anterior compartment is supplied by branches of the femoral nerve and the sciatic nerve by way of the tibial and common peroneal nerves. Among these multiple branches are the 4 main genicular branches, which are named for the corresponding quadrants of the knee joint: superolateral genicular nerve (SLGN), superomedial genicular nerve (SMGN), inferomedial genicular nerve (IMGN), and inferolateral genicular nerve (ILGN).7
The genicular nerve block generally targets 3 locations: SLGN, SMGN, and IMGN, however some studies have shown utility in also blocking the nerve to vastus intermedius (NVI).8 The ILGN and the recurrent peroneal nerve, which innervate the inferolateral aspect of the knee joint, are excluded from this block because of their close proximity to the common peroneal nerve, which could potentially cause a transient foot drop if blocked.9
The SLGN arises from the peroneal nerve and it winds around the femur to the junction between the lateral epicondyle and the shaft of the femur. At this junction the SLGN innervates part of the anterolateral periosteum and capsule. The SMGN is a branch extending off the tibial nerve and it travels close to the adductor tubercle to innervate the anterior medial knee joint. The IMGN also arises from the tibial nerve and courses to the junction of the tibial shaft and the medial tibial condyle, where it then innervates the rest of the anteromedial knee joint. Lastly, the NVI, a branch of the femoral nerve, lies on the anterior aspect of the femur just proximal to the patella.
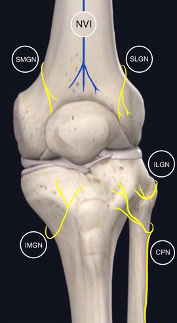
Figure 1: Superolateral genicular nerve (SLGN), superomedial genicular nerve (SMGN), inferomedial genicular nerve (IMGN), inferolateral genicular nerve (ILGN), nerve to vastus intermedius (NVI), and common peroneal nerve (CPN).
Analgesia
The distribution of analgesia corresponds to the general location of the targeted genicular nerves. Given this nerve block’s easily identifiable landmarks and ability to provide motor-sparing analgesia, it can be a useful tool for emergency physicians when treating acute knee pain in the emergency department (ED).
Technique
A high frequency linear probe is used and placed on 4 separate locations to target the SMGN, SLGN, and IMGN (Figure 2A). The probe is placed at an oblique angle to obtain a sagittal view of the distal femur and proximal tibia. The needle is advanced toward the knee for all three injections. As with all nerve blocks, aspiration should be done before every injection to avoid inadvertent intravascular injections.

Figure 2: Probe and needle orientation for SLGN, SMGN, IMGN, NVI (from left to right)
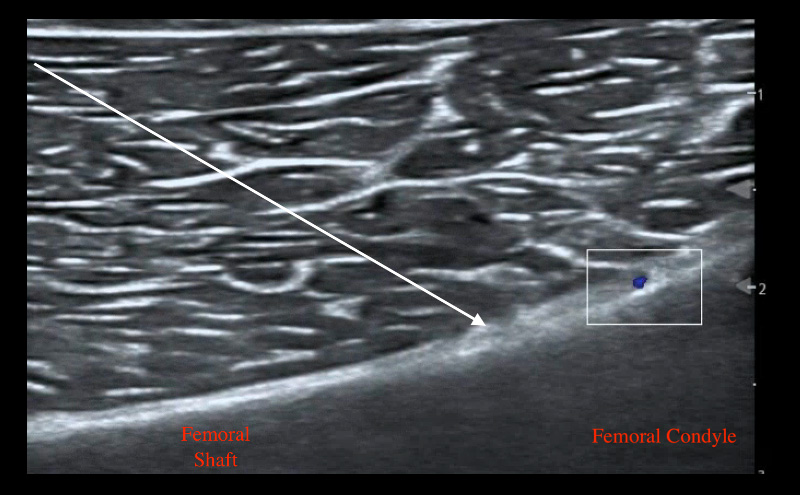
To target the SMGN, place the transducer on the medial aspect of the distal femur with the probe marker facing superiorly and identify the femoral shaft and femoral condyle. Another approach would be starting at the knee joint and moving superiorly to identify the femur bone. As the femoral shaft slopes superiorly, place color Doppler to identify the superior medial genicular artery. Advance a 20 gauge needle (or smaller) toward the slope avoiding the artery and make contact with bone. Inject 3-5 mL of local anesthetic lifting soft tissue and spreading along the periosteum.
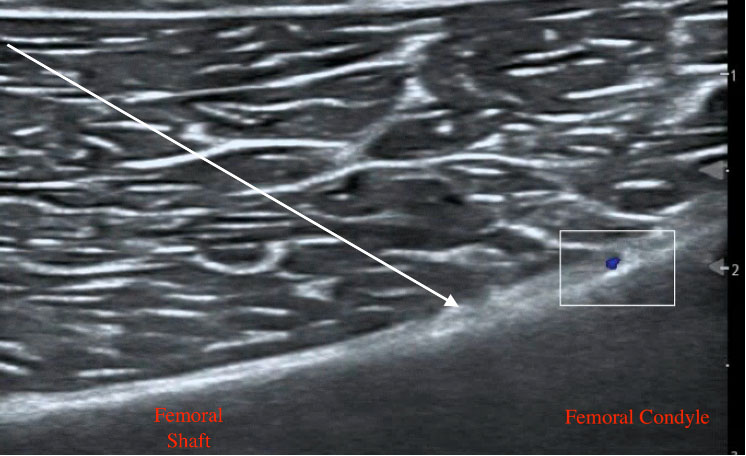
Figure 3: SMGN ultrasound anatomy with needle trajectory indicated by arrow
The SLGN block is performed with the same technique as for the SMGN, but by placing the transducer on the lateral aspect of the femur (figure 2).
To block the IMGN, place the linear probe on the superomedial aspect of the tibia and identify the tibial shaft and medial condyle. Place color Doppler where the shaft slopes up to become the condyle and identify the inferior medial genicular artery. Advance the needle toward the knee making contact with the shaft as it slopes upwards and inject 3-5 mL of local anesthetic.
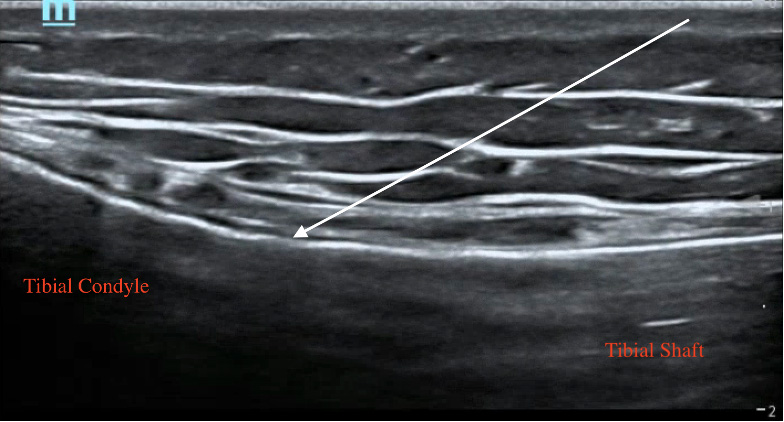
Figure 4: Tibial ultrasound anatomy with arrow indicating needle trajectory
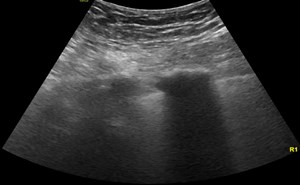
To block the nerve to vastus intermedius (NVI), place the linear probe 3-5 centimeters above the patella and get a short axis view of the distal femur. Advance the needle until it makes contact with the bone and inject 3-5 mL of local anesthetic.
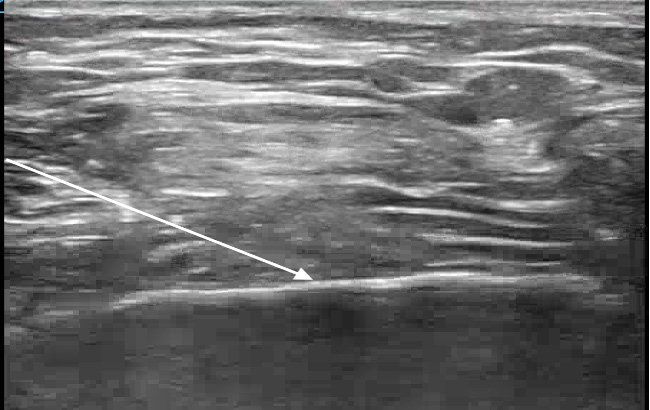
Figure 5: Distal femur in short axis with arrow indicating needle trajectory for NVI block
Discussion
The genicular nerve block is a useful method to provide analgesia for acute or acute-on-chronic knee pain in the ED. Not only is this block safe and effective, it also spares motor function by selectively targeting the sensory branches of the anterior compartment of the knee. This technique may be used as an adjunct
to traditional methods of pain relief or on its own to avoid the side effects of systemic analgesia. Although the genicular nerves are not directly visualized on ultrasound given their small size, ultrasound guidance provides recognizable anatomic landmarks to reliably infiltrate the target location. Using an adequate volume of local anesthetic can help avoid inconsistent analgesia.
As ultrasound-guided nerve blocks are increasingly incorporated into practice in the ED and as emergency physicians become more comfortable with the technique, the genicular nerve block may prove to be a useful new tool to treat knee pain in this setting.
References
- Choi W-J, Hwang S-J, Song J-G, et al. Radiofrequency treatment relieves chronic knee osteoarthritis pain: a double-blind randomized controlled trial. PAIN®. 2011;152(3):481-487.
- Demir Y, Güzelküçük Ü, Tezel K, Aydemir K, Taşkaynatan MA. A different approach to the management of osteoarthritis in the knee: Ultrasound guided genicular nerve block. Pain Medicine. 2017;18(1):181-183.
- Sahoo RK, Krishna C, Kumar M, Nair AS. Genicular nerve block for postoperative pain relief after total knee replacement. Saudi J Anaesthesia. 2020;14(2):235.
- Caldwell Jr GL, Selepec MA. Reduced opioid use after surgeon-administered genicular nerve block for anterior cruciate ligament reconstruction in adults and adolescents. HSS Journal. 2019;15(1):42-50.
- Howell R, Hill B, Hoffman C, Treacy E, Mulcahey MK. Peripheral nerve blocks for surgery about the knee. JBJS reviews. 2016;4(12):e1.
- Sobel J, Oswald J. Novel use of 3-point genicular nerve block for acute knee pain in the emergency department. J Emerg Med. 2021;61(4):416-419.
- Dunworth S, Gadsden J. How I do it: genicular nerve blocks for acute pain. ASRA Pain Medicine News. 2022;47.
- Wong PKW, Kokabi N, Guo Y, et al. Safety and efficacy comparison of three- vs four-needle technique in the management of moderate to severe osteoarthritis of the knee using cooled radio frequency ablation. Skeletal Radiol. 2021;50(4):739-750.
- Tan, Y. K., Neo, E. J. R., & Wee, T. C. Ultrasound-guided Genicular Nerve Blockade With Pharmacological Agents for Chronic Knee Osteoarthritis: A Systematic Review. Pain Physician. 2022;25(4):E489–E502.